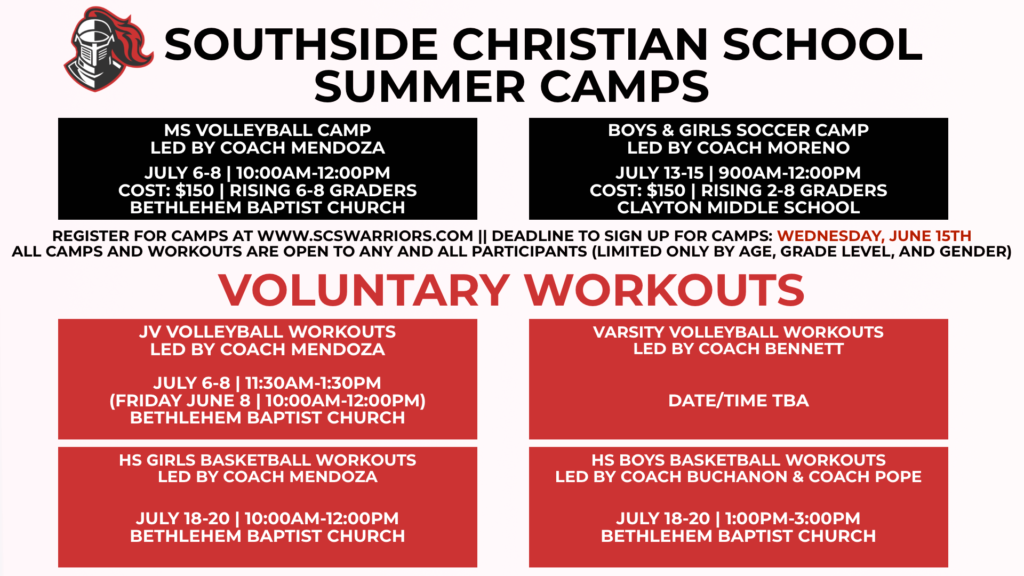
2022 Summer Sports Camp The Registration Form is below the Informational Flyer. Please enable JavaScript in your browser to complete this form.Student Athlete's Name *FirstLastHome Address *Parents' Names *Parent Email *Parent Phone Number(s) *Student Date of Birth *Student Grade for 2022-23 school year *For which camp(s) are you registering your student athlete? *MS Girls Volleyball (6th-8th grades ) $150Boys and Girls Soccer (2nd-8th grades) $150T shirt size for your student athlete *YSYMYLASAMALWho is allowed to pick up your child from sports camp? *Emergency Contact Person's Name and Phone Number (if other than parents listed above)Health Insurance Carrier *Policy Number *Under the Name of: *Relationship to Student *Date of Last TetanusPreferred HospitalAllergies (including reactions to medication)Are there any physical or medical conditions we should know about not already stated?Medications being taken currently:BY TYPING YOUR NAME BELOW AFTER READING, YOU UNDERSTAND AND AGREE TO THESE STATEMENTS AND THAT THIS FORM OF ELECTRONIC SIGNATURE HAS THE SAME LEGAL FORCE AND EFFECT AS A MANUAL SIGNATURE. Although the school desires to provide a safe and enjoyable time for all students, accidents can still happen. I/we understand that there are risks/dangers involved with participation in camp activities. In consideration of my child being allowed to participate in this event, I/we assume responsibility for those ordinary and reasonable risks associated with the activities. I/we agree to hold harmless Southside Christian School, its affiliated organizations, employees, agents, and representatives, including volunteer and other drivers, from any and all claims arising from my child’s participation. This release agreement does not apply to claims of intentional (criminal) misconduct or gross negligence by the school, its employees, or volunteers. If such circumstances are proved in a court of law, I/we acknowledge and agree that the school can assume no financial liability beyond its actual liability insurance policy in force. In case of accident, illness, or other emergency, I/we request that the school contact me. If the school cannot reach a parent/guardian after conscientious effort, I/we give permission for school staff to call paramedics or any licensed physician or dentist. If a life-threatening emergency exists, I/we give permission for school staff to immediately call paramedics and then contact me/us as soon as possible thereafter. I/we authorize and consent to any X-ray examination, anesthetic, medical, dental, or surgical diagnosis or treatment, and hospital care which, in the best judgment of a licensed physician or dentist, is deemed advisable. I/we agree to assume the financial responsibility for expenses incurred as a result of those services being provided. I/we also agree to be financially responsible for emergency medical transportation. *Is there any additional information you would like to include?Submit